Learning about normal work is the key to understanding how all events, wanted and unwanted, occur!
Traditional Approach
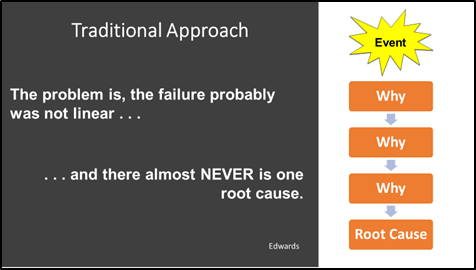
Traditional methods of investigation focus on a linear process to determine a root cause and require the investigator to remove context to gain understanding. However, failure in complex systems is not linear and the understanding of context is a pre-requisite of just about all valid forms of scientific investigations.

A major shortcoming with root cause analysis is that it limits the scope of the investigation to the event itself. There is no room to examine variability, structured thinking is encouraged, and some methods directs the investigator to preconceived outcomes. This often focuses on the people involved at the time of the incident and excludes everything else that is going on around it.
Blue line vs Black line

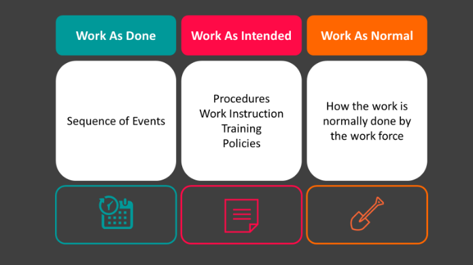
Most organisations have systems, procedures, policies which instruct workers on how to undertake specific tasks. Recently we have referred to this as “Work as Imagined”, “Work as Intended” or the “Black Line”.
In reality, humans are complex adaptive beings and will adapt the work to get the task completed. Workers come to work with every intention of completing their tasks and no intention at all of injuring themselves. The way this work is completed we call the “Blue Line”.
Conditions such as production pressure, lack of tooling, equipment breakdowns, errors, fear of reporting, change of plans, flawed processes, design shortcomings, goal conflicts, trade-offs and more all contribute to how work is normally completed. Workers will work around these conditions to get the job done.
All these conditions represent the context of the work, they always exist, and the vast majority of the time work is successful. Only when they align in a certain way do we then get an event or a near miss.
Most organisations have robust investigations processes in place to capture the information surrounding an event. They take statements of people involved and witnesses. They take photographs of the incident scene and may do re-enactments. They will compare this information to the procedures and polices in place. Rarely do we look at how the task is normally completed throughout an organisation and chances are, this is where the systemic issues lie.
The key to understanding
To truly understand an event, we need to focus, not just on the “Why?” but the “How?”
To do this we need to understand how the work is normally undertaken and compare it to how the work was intended by the organisation to be completed and the circumstances of the event itself.
Gathering the information to learn
Most organisations have robust investigations processes in place to capture the information surrounding an event. They take statements of people involved and witnesses. They take photographs of the incident scene and may do re-enactments. They will compare this information to the procedures and polices in place. Rarely do we look at how the task is normally completed throughout an organisation and chances are, this is where the systemic issues lie.
Capturing “Work as Normal”
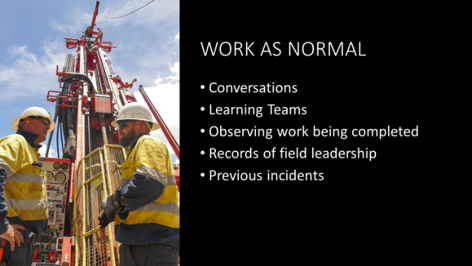
This information can not just be captured in a room. We need to get out in the field and have conversations with our people. We need to focus on the task itself. (Not the paperwork. How do they complete the task compared to others? How do the rest of the team do the task? How do other shifts or sites do it? What about night shift? Use a variety of methods to learn about normal work.
Operational Learning Questions
Ask questions designed to promote conversation and storytelling. Focus on the task, not on the paperwork.
- Tell me about your work.
- What does a bad day look like?
- What does a good day look like (for this process)?
- What is the worst thing that could happen in this process / area?
- What is very unpredictable?
- What near misses have we had?
- How far back in the process should we start for us to understand?
- Do you have the right tools?
- What is very predictable?
- Where is it easy to make a mistake?
After the Event
Again, focus on the conditions of the task.
- What did you hear/see/think?
- What else should I know?
- Was there anything different before or at the time of the event?
Let’s put it all together
Create a 3 tier timeline or sequence of events as per the example below.
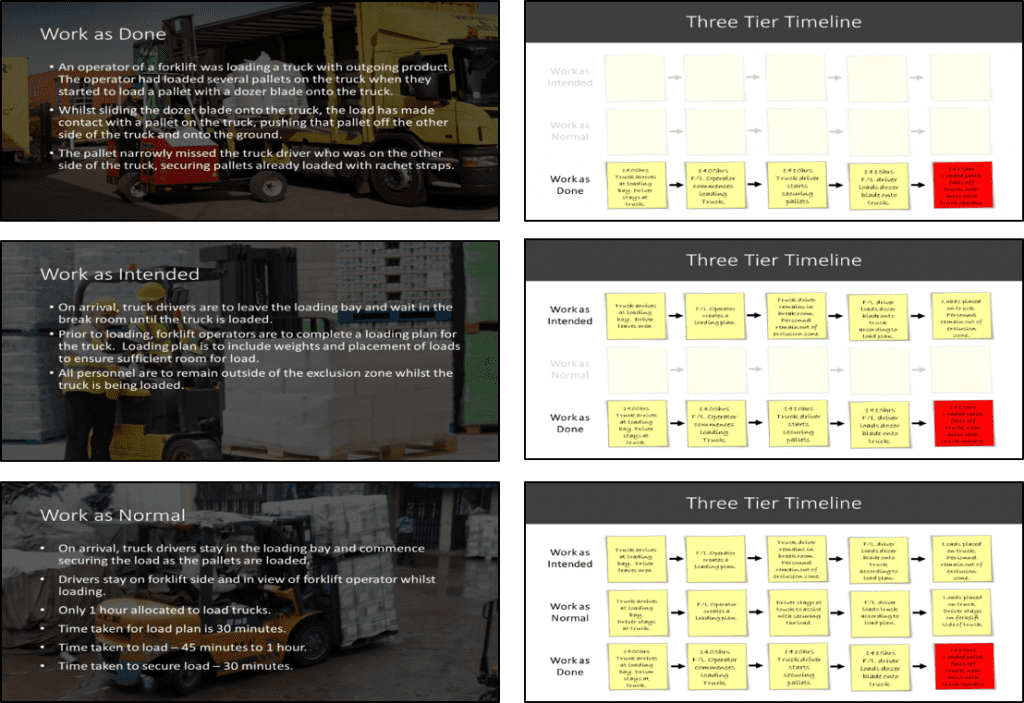
Identify and investigate the gaps or differences
Where is does work as normal vary from works as intended? Explore and investigate all the differences.

Corrective Actions
We can not hope to fix every possible issue or concern that was identified. Use your organisation’s risk management process to prioritise actions. Actions should be focused on the task and not on procedures. Re-training, toolbox talks, and discipline will never prevent an event from occurring.
Although our actions are no guarantee an incident won’t be repeated, it should not occur again from the issues identified in the investigation.